Bone metastases are a phenomenon of secondary cancer in which cancer cells migrate to bone tissues and form malignant tumors. Metastasis occurs in the late stages of cancer development and is accompanied by pain, increased levels of calcium in the blood plasma, impaired blood flow and fractures.
Causes
The appearance of mts (metastases) in the bones is due to the spread of cancer cells through the blood vessels from the primary affected organ to the bone tissues, developing into malignant tumors. Most often they migrate from the initially affected thyroid and mammary glands, lungs, kidneys, as well as with Sarcomas, and. Less common are metastases from the cervix, ovaries, gastrointestinal tract, and soft tissues, and very rarely from other organs. The most common localization is metastases in bones with abundant blood supply: the bones of the pelvis, arms, legs, chest, skull, bone marrow and ribs. Not infrequently, metastases are found in the hip joint, shoulder and knee joints. With breast cancer in women, with, kidneys and lungs, metastases can go to the xiphoid process, body and handle of the sternum, as well as to the ilium, ribs, pelvic, hip bones and shoulder bones.
Tumors disrupt the work of osteoblasts and osteoclasts - large multinucleated cells responsible for regulating the structure and destruction of bone tissue in the process of cell renewal.
Surgery, pathological fractures, and other complications of metastasis can cause chilostasis (lymph stasis), leading to edema. Bone metastases can cause severe pain, such as spinal melanoma or ischial tumors that can compress a nerve.
Leading clinics in Israel
The main symptoms are hypercalcemia, pathological fractures, and spinal compression. There is also an increased temperature due to the active metabolic process and accelerated cell division.
Hypercalcemia
In a third of patients, bone metastases cause hypercalcemia. Calcium, which is part of the bones, is released during bone erosion and enters the bloodstream. Hypercalcemia causes a number of symptoms:
Nervous system:
- Mental instability;
- lethargy;
- Depression;
- Disorder of mental activity.
The cardiovascular system:

- Lack of appetite;
- Nausea;
- Vomit;
- Ulcerative formations.
Urinary system:
- increased urine production;
- kidney failure;
- Intoxication.
pathological fractures
The area of the bone affected by metastases becomes fragile due to a malfunction of osteoblasts and osteoclasts, which leads to pathological fractures. Pathological fractures appear if more than half of the outer bone layer is damaged. A fracture may provoke a mild blow, or there may be no obvious cause at all. Metastatic lesions most often affect the femur, thoracic and lumbar spine.
Spinal compression
 Up to 5% of patients with mts in the spine develop spinal compression, of which in more than half of the cases, metastases are found in the thoracic spine. A growing tumor or bone fragments from a fracture can compress the spinal cord, leading to often irreversible paralysis if the damage is not detected in time. In the case of already developed paralysis, only one out of ten patients manages to restore motor function.
Up to 5% of patients with mts in the spine develop spinal compression, of which in more than half of the cases, metastases are found in the thoracic spine. A growing tumor or bone fragments from a fracture can compress the spinal cord, leading to often irreversible paralysis if the damage is not detected in time. In the case of already developed paralysis, only one out of ten patients manages to restore motor function.
If compression was facilitated by a gradual increase in the tumor, then signs of compression of the spinal cord are not noticed for a long time, in contrast to the case when a shifted fragment of a vertebra leads to compression.
Kinds
Osteoblasts and osteoclasts are the main cells involved in normal bone renewal. With metastases in the bones, allostasis is disturbed (the body's ability to respond to atypical changes and carry out homeostasis - self-regulation), because of which the cells begin to work with a pathological bias, the body cannot cope with the regulation of cellular processes, and a subtotal lesion occurs in the bones.
osteoblastic
Osteoblasts are the building blocks of the skeleton that fill empty areas, produce extracellular substance (matrix) and turn into bone tissue cells (osteocytes). If osteoblasts fail due to metastases in the bones, then osteosclerotic foci (otherwise sclerotic, i.e. seals) form in the bones - such disorders are called osteoblastic or blastic, and the formation of seals is an osteoblastic process.
osteolytic
 Osteolytic refers to disorders in the bones, in which the destruction of bone tissue occurs. What it is? Osteoclasts break down bone tissue to allow new bone cells to form. Failure in their work leads to an uncontrolled destructive process in which holes are formed in the bones. Bones become brittle and brittle, easily broken and cracked.
Osteolytic refers to disorders in the bones, in which the destruction of bone tissue occurs. What it is? Osteoclasts break down bone tissue to allow new bone cells to form. Failure in their work leads to an uncontrolled destructive process in which holes are formed in the bones. Bones become brittle and brittle, easily broken and cracked.
Bone metastases are rare, resulting in a single type of damage and the manifestation of damage is most often of a mixed type, with signs of both tissue compaction in separate areas and destruction.
Diagnostics
To check for the presence of metastases, there are a number of procedures for diagnosis at different stages of the development of the disease:
- Scintigraphy - an examination by injecting radioactive isotopes to obtain a two-dimensional image, where lesions appear that look like white spots. Helps to learn about the presence of metastases at an early stage of their development;
- Radiography - allows you to identify the nature of the lesion, noticeable only in the later stages;
- Computed or magnetic resonance imaging gives a three-dimensional image of the skeleton;
- Biochemical blood test to check the level of calcium in the blood plasma and diagnose hypercalcemia;
- Biopsy - allows you to accurately determine the malignancy of neoplasms and make a final diagnosis.
Treatment
Treatment is prescribed by an oncologist based on blood test data, localization of primary and secondary cancers, the stage of destruction and the type of bone damage (osteoblastic and osteolytic are treated differently). The main direction of treatment is to eliminate severe complications to improve the patient's quality of life. If the spine and bones hurt, then they resort to anesthesia. How to treat metastases, the oncologist determines after all the necessary diagnostic procedures.
 Treatment consists of medications such as hormones, bisphosphonates, immune-boosting drugs, and topical procedures such as radiation and surgery. Painkillers are prescribed to relieve pain. Folk remedies include decoctions of herbs, poultices, including folk remedies for pain, for example, an ointment from the root of comfrey, which is treated by applying to a sore spot.
Treatment consists of medications such as hormones, bisphosphonates, immune-boosting drugs, and topical procedures such as radiation and surgery. Painkillers are prescribed to relieve pain. Folk remedies include decoctions of herbs, poultices, including folk remedies for pain, for example, an ointment from the root of comfrey, which is treated by applying to a sore spot.
Operation
Surgery is performed if there are serious complications, such as a fracture, spinal compression, loss of limb mobility or paralysis. Operatively, tumor-like formations are removed. If it is necessary to restore the bone structure, supporting pins and plates are installed. The operation is indicated to be done with a favorable picture of the disease and a good general condition of the patient. Otherwise, it is recommended to use fixation devices to support the bones.
Titanium is recommended for osteosynthesis (bone fusion by means of metal alloys) to avoid metallosis - metal oxidation and penetration of its particles into the muscle tissue. With severe bone deformity after removal of the tumor in some clinics, a plastic surgeon performs plastic surgery on the bone or endoprosthetics of the joints.
Chemotherapy
Chemotherapy and radiation therapy are prescribed to destroy cancer cells and prevent further development of metastases. and irradiation prepares the patient for surgery and supports after it. called transillumination with ionizing radiation, which destroys cancer cells, or the introduction of strontium-89 or samarium-153 preparations. Post-radiation complications require rehabilitation at the end of the course.
Treatment with bisphosphonates
 Bisphosphonate drugs are of great help in slowing down secondary changes (secondary cancers) in general and bone destruction in particular by suppressing the uncontrolled work of osteoblasts and providing a balance between the destructive and regenerative process.
Bisphosphonate drugs are of great help in slowing down secondary changes (secondary cancers) in general and bone destruction in particular by suppressing the uncontrolled work of osteoblasts and providing a balance between the destructive and regenerative process.
Want to get a quote for treatment?
Bisphosphonate drugs include:
Nitrogen containing bisphosphonates:
- pamidronate;
- Ibandronate.
Nitrogen-free bisphosphonates:
- Tidronate;
- Clodronate;
Drugs containing nitrogenous compounds have a greater therapeutic effect than bisphosphonates without nitrogen.
Immunotherapy
Immunity boost is used to recognize and fight cancer cells. Immunity-boosting drugs increase the amount of immune antibodies and increase their ability to recognize and kill cancer cells.
How long do they live with bone metastases
 Life expectancy with bone metastases directly depends on the location of the foci from which the cancer cells were transferred. In general, a time corridor of life expectancy has been determined for each type of cancer, but this period is not a sentence, because in some cases the situation depends on the presence and degree of complications and it is possible to stop the destructive processes.
Life expectancy with bone metastases directly depends on the location of the foci from which the cancer cells were transferred. In general, a time corridor of life expectancy has been determined for each type of cancer, but this period is not a sentence, because in some cases the situation depends on the presence and degree of complications and it is possible to stop the destructive processes.
Prevention
Bone metastases are less dangerous than metastases to the sternum and abdominal organs. It is recommended to reduce the load on the affected areas of the skeleton as much as possible, use crutches depending on the location of the metastases, lie down more often, wear a supporting corset or head support and not lift weights. Nutrition should include foods that are good for bones and overall immunity.
Can bone metastases be cured? Early detection of metastases and strict adherence to the treatment and recommendations prescribed by the doctor increases the chances of defeating the disease and saving the patient's life.
Video: Bone metastases
Anonymous reviews
Anonymously. A friend was diagnosed first with breast cancer, then with lytic metastases. The doctor told her that they live with MTS for a long time, a friend goes every month to drip Zometa and, in general, feels good.
Anonymously. The doctor also told me that the survival rate with mts in the bones is higher than if in the organs. There were two chemo, now I take bisphosphonates regularly and I continue to live a full life, so there is no need to despair.
Anonymously. The grandmother with metastases lived for 10 and a half years, but there were pains and several fractures, she is active, she did not sit still. She took morphine for pain.
Metastatic bone disease
Bone metastases are an extremely common complication of advanced cancer. Most often they are found in patients with cancer of the breast and prostate glands, as well as with cancer of the kidney, lung, lymphomas. Bone metastases lead to serious complications such as severe pain, bone fractures, life-threatening fluid and electrolyte imbalance, and spinal cord or nerve root compression syndrome. Management of patients with bone lesions is often very difficult, as severe pain and neurological changes are often difficult to treat and lead to a significant deterioration in the quality of life of patients. Bone metastases indicate the presence of widespread, i.e. incurable process, but with a fairly active complex treatment, it is possible to achieve not only an improvement in the quality of life, but also a significant extension of it.
Types of bone metastases
Depending on the processes prevailing in the bone, osteolytic and osteoblastic metastases are distinguished. An osteolytic lesion means that the tumor destroys the bone, which appears to be melting or dissolving. This is due to the loss of calcium from the bone. On x-rays, this process looks like holes inside the bone. The osteolytic type of lesion is most characteristic of a malignant disease called multiple myeloma. Osteoblastic lesion, on the contrary, is manifested by an increase in bone tissue production at the site of the lesion. The tumor sends signals to the bone that result in an overproduction of bone cells, creating stiff, rigid, altered bone. A typical variant of the osteoblastic focus are cancer metastases. prostate. In most cases, with other types of tumors, one of the types of lesions is observed - osteolytic or osteoblastic, but mixed metastatic foci occur. In patients with breast cancer, as a rule, osteolytic foci occur, and only 15-20% of patients develop osteoblastic lesions.
Why are bones affected?
The skeleton is a fairly common place for the formation of metastatic foci, not only in patients with prostate and breast cancer, but also in the lungs, kidneys, stomach, Bladder, uterus, thyroid gland, colon and rectum. Researchers suggest that frequent bone damage is associated with intense blood flow in the bones and bone marrow. When cancer cells gain access to blood vessels, they can migrate into the body. They usually go where the blood flow is more intense. In addition, tumor cells themselves can secrete adhesive molecules that form bonds with bone matrix and bone marrow cells. Interactions with these tumor molecules result in signals that lead to increased bone destruction and accelerated tumor growth in the bones. Held in last years Research has shown that bones are the source of many of the factors that induce cells to divide, grow, and mature. When a bone is damaged by cancer cells, many of these factors are released, which stimulate the growth of tumor cells in the future. This interaction leads to a vicious cycle, supporting bone destruction and tumor growth.
Symptoms of bone metastases
The initial symptoms of bone metastases are often difficult to recognize and masquerade as various conditions. Most patients who develop problems associated with bone metastases note that symptoms that have occurred in the past could be due to many reasons. The most common symptom is pain in the back, limbs, and other places, which are often mistaken for manifestations of osteochondrosis, arthrosis, etc. Bone fractures without previous trauma are also common. There may be violations of the function of the large intestine and bladder - both urinary or stool incontinence (more common), and severe constipation or urinary retention. Other patients may notice weakness and / or decreased sensation in the legs, incoordination of movements and a feeling of their greater severity. The last symptoms are very serious, they indicate that the tumor has spread to the spinal cord and compresses the nerve roots. Such conditions require immediate treatment. A rarer manifestation of metastatic disease is an increase in serum calcium levels, leading to constipation, abdominal pain, and in more severe cases, loss of consciousness.
If you experience pain in the back or in the limbs, be sure to contact your doctor, who will prescribe an appropriate examination. Do not start with consultations of chiropractors and neuropathologists, who, not knowing about your past oncological disease, may prescribe you massage or electrical procedures, which are strictly prohibited for oncological patients. In addition, taking painkillers and not receiving special treatment, you are wasting your time. The sooner you start treatment for bone metastases, the more likely you are to be successful.
Diagnosis of bone metastases
Currently, there are many studies that allow the detection of bone metastases when patients have corresponding complaints. In some cases, it is possible to diagnose a metastatic lesion before symptoms appear. Doctors use x-rays, bone scans (osteoscintigraphy), and magnetic resonance imaging (MRI) to diagnose this type of tumor spread. Conducting a conventional x-ray examination is most useful and informative in the presence of a predominantly lytic type of lesion. Such foci on radiographs look like a "hole" or dark spots against a background of relatively normal bone tissue. Unfortunately, X-ray examination is informative only in cases where the tumor has destroyed a significant part of the bone tissue. In contrast, bone scans can detect bone metastases very early. This test consists of intravenously injecting a small amount of a radioactive substance with a very short decay period. The rays emitted by this source are fixed by a special crystal some time after the injection. The substance with which the emitter is associated accumulates mainly in the foci of the metastatic process, looking out on the image as brighter areas (increased drug accumulation density). Due to the high sensitivity of the method, it is sometimes difficult to distinguish arthritis, some infectious processes, sites of old fractures from a true tumor focus. Bone scanning is also used to monitor the effectiveness of the treatment of patients with an already identified metastatic process. CT scan sometimes it can also show metastatic bone disease. Magnetic resonance imaging is more useful in studying the condition of the nerve roots, if they are suspected of being squeezed by a tumor or bone fragments due to their destruction by a tumor. More often, MRI is used for suspected compression of the spinal cord. Recently, a completely new diagnostic method has appeared - pseudoPET or MRI in the "whole body" mode, which allows early detection of minimal lytic foci in the skeleton.
Until recently, there was no blood test that could be used to diagnose bone metastases. But over the course of several years, studies have been carried out that have revealed a significant increase in the serum level of one of the enzymes that is specific for bone metastases. It is called tartrate-resistant acid phosphatase. It has been proven that changes in its concentration appear before radiographic changes, in addition, a decrease in the level reflects the effectiveness of the treatment. For example, an increase in calcium levels or an enzyme called alkaline phosphatase may be associated with the presence of bone metastases, but these data alone are not enough to make a diagnosis.
Treatment
The main method of treatment of metastatic bone lesions is the treatment of the primary tumor. Therapy may include chemotherapy, hormone therapy, radiation therapy, including radiosurgery, immunotherapy, or treatment with monoclonal antibodies. Narcotic and non-narcotic analgesics (NSAIDs) are used to treat pain. Currently, there are a large number of painkillers, including combined ones, consult your doctor for which drug should be preferred. In addition, there is no need to be afraid (if necessary, caused by pronounced pain syndrome) take drugs for a while. American studies have shown that people who take drugs for chronic pain almost never become drug addicts. Prescribing drugs is not a sign that further treatment is inadvisable, but an attempt to improve your general condition until such time as special antitumor therapy takes effect.
Surgical intervention may be necessary if there is a threat or presence of a fracture of bones or vertebrae, as well as in cases where the tumor affects the nerves and nerve roots. In recent years, the use of a minimally invasive technique called puncture vertebroplasty has also spread. Its essence lies in the introduction of a special polymer through a needle into the affected vertebra, which cements and strengthens the vertebrae, preventing the occurrence of fractures and related serious neurological problems.
Radiation therapy is the traditional means of pain relief for metastatic skeletal lesions. Local irradiation reduces the severity (intensity) of the pain syndrome in about 80% of patients, more than 50% of patients note the complete disappearance of pain in the area that was irradiated. In addition, radiation therapy makes it possible to achieve consolidation (remineralization) of pathological fractures and is an effective means of combating compression syndrome (compression of the nerve roots or spinal cord by a tumor. The duration of the course of analgesic radiation therapy is determined by the characteristics of a particular clinical case - this can be a single exposure a rather large dose, or a longer course of treatment (irradiation is carried out from 4 to 12 times).A breakthrough in the treatment of metastatic lesions of the spine was the use of CyberKnife, which allows you to deliver a large dose sufficient to eradicate the tumor without damaging the spinal cord and nerve endings.
Currently, with multiple bone metastases in patients with breast and prostate cancer, phosphorus-32 and strontium-89 are widely used for the treatment, however, this method of therapy is associated with a high level of pronounced myelosuppression (suppression of hematopoiesis by the red bone marrow). More popular is the use of samarium-153, which has a rapid analgesic effect, with significantly lower myelosuppression than traditional radiopharmaceuticals.
It also gives positive results from the use of hormone therapy - it increases the duration of the relapse-free period and improves the quality of life of patients, primarily those with breast and prostate cancer. A more pronounced analgesic effect has a combination of bisphosphonates with hormone therapy, especially in the treatment of patients with breast cancer and multiple myeloma.
Recently, there has been an increasing use of new class medicines - bisphosphonates, designed to treat pain caused by bone metastases, and which can restore bone structure.
Depending on the characteristics of your clinical case, the doctor will choose the optimal combination of antitumor effects for you.
Bisphosphonates
Bisphosphonates are a group of drugs that reduce the intensity of pain in metastatic bone disease and improve the overall structural condition of the bones. Bisphosphonates are analogues of a natural component of bone called pyrophosphate and prevent fractures. This class of drugs is widely used to treat and prevent osteoporosis and certain other bone disorders (such as Paget's disease), as well as elevated serum calcium levels (a condition called hypercalcemia). Bisphosphonates inhibit the destruction of bone by cells called osteoclasts, and can also (indirectly stimulate the formation of new bone structure by affecting cells called osteoblasts. According to the above, and based on the results of many clinical studies, bisphosphonates are one of the most effective drugs for reducing pain in metastatic bone disease, thanks to them, a significant place is allocated in the treatment of this group of cancer patients.Unfortunately, bisphosphonates are not considered as a means of radical treatment.It has been proven that bisphosphonates prevent the occurrence of severe and serious complications of metastatic bone disease and can increase the survival of patients with lytic foci most researchers agree that these drugs are more effective and useful as a means of restoring bone structure, in the presence of osteolytic lesions and, somewhat less, in osteoblastic them metastases. At the same time, bisphosphonates are able to effectively reduce the intensity of pain in both types of lesions.
There are oral (tablet) and infusion (intravenous) bisphosphonates. Some oncologists prefer intravenous administration once a month, considering it more convenient for patients, others prefer long-term oral administration, believing that this regimen is more favorable for restoring bone structure.
Depending on the type of tumor you have and the type of metastatic lesion, as well as certain biochemical parameters (eg, serum calcium levels), your doctor will prescribe certain drugs and the regimen for their use. The results of many studies have shown that the use of bisphosphonates provides significant benefits in the treatment of patients with metastatic bone disease, so when observed for six months, bisphosphonate therapy leads to a 35% reduction in the risk of fractures of the vertebrae and other bones, and the risk of such a serious, life threatening, conditions such as hypercalcemia, the need for radiation therapy decreases. Studies with a follow-up period of more than one year have also shown a reduction in the need for orthopedic surgery.
It should be noted that the effect of bisphosphonates is better the earlier they are started to be used, i.e. they should be prescribed immediately upon detection of bone lesions. It has also been proven that the duration of the use of drugs should be at least 6 months. The dependence of the severity and duration of the clinical effect on the duration of taking bisphosphonates has been established - that is, the longer the better. In addition, their intake significantly increases the time before the occurrence of complications of metastatic bone disease.
Long-term use of bisphosphonates prevents the formation of new bone lesions not only in patients with breast cancer and multiple myeloma, but also in patients with prostate cancer.
One of the complications of cancer is that it can spread to soft tissues and distant organs.
Metastasis occurs in the bones. In fact, bone metastases are secondary cancerous tumors of the bone tissue, which are formed as a result of the transfer of atypical cells from the main focus with the bloodstream and lymph flow.
Usually, bone metastases occur already at the last stages of oncopathology. Moreover, about 80% of cases of bone metastasis occur against the background of and. Such formations are manifested by severe pain, frequent fractures and hypercalcemia.
Causes
Most often, metastasis to bone structures occurs with and, prostatic and breast cancer, malignant tumors in and gastrointestinal structures, and.
Metastasize to bone tissue and other malignant neoplasms, only much less frequently.
When a person is healthy, his bones are constantly being renewed. In general, bone structures are characterized by the processes of resorption, remodeling and bone formation. These processes are carried out due to the cellular activity of osteoblasts and osteoclasts. These cellular structures are responsible for the formation, absorption and destruction of bone tissue.
If atypical cells penetrate into the bone structures, then there is a violation of the functioning of the bones. Healthy cells are displaced, the processes of interaction between osteoblasts and osteoclasts are disrupted, which leads to the uncoupling of their activity.
For breast cancer
Metastasis to bone structures in breast cancer occurs in the lymphogenous and hematogenous way. Such localization of metastases in breast cancer is quite common.
Cancer with such metastases is characterized by severe morbidity and an excessive tendency to pathological fractures, especially in chest And pelvic bones.
Types
Depending on the type of cell activation, oncologists distinguish several types of bone metastases:
- Osteoplastic- accompanied by the formation of seals on the bones;
- osteolytic- when there is a predominant destruction of bone structures.
Pure types in medical practice are relatively rare, their mixed forms are much more common.
The most susceptible to metastasis are bones that have a rich blood supply, i.e., in the shoulder and femur, ribs and vertebral, cranial and pelvic bones. At first, bone metastases do not manifest themselves in any way, but over time they cause intense pain, which is associated with stimulation of pain periosteal receptors.
Symptoms of bone metastases
 At first, bone secondary tumors develop asymptomatically, but with the development of the tumor process, a certain clinical picture is formed:
At first, bone secondary tumors develop asymptomatically, but with the development of the tumor process, a certain clinical picture is formed:
- The presence of hypercalcemia;
- Tendency to pathological fractures;
- The presence of spinal compression.
Hypercalcemia is a life-threatening complication that is found in about 30-40% of cancer patients with bone metastasis.
This condition occurs due to excessive activity of osteoclasts, leading to an increase in the level of calcium in the blood, which in turn causes a pathological increase in renal excretory abilities.
As a result, in cancer patients with bone metastases, in addition to hypercalcemia, hypercalciuria develops, the reverse absorption of fluid and sodium is disturbed, leading to polyuria.
As a result of such changes in cancer patients, the activity of many systems and organs is disrupted:
- In the nervous system activity, signs such as lethargy and mental disorders, confusion in the mind and affective disorders are noted;
- In cardiovascular activity, abnormalities occur, such as arrhythmia and low blood pressure, a decrease in heart rate, while the risk of cardiac arrest is high.
- The kidneys are affected by nephrocalcinosis and polyuria;
- In the gastrointestinal area, there is a nausea-vomiting syndrome, frequent constipation and lack of appetite, or pancreatitis may develop.
If more than half of the cortical layer is destroyed during bone metastasis, then pathological fractures appear. They are usually found in the bones of the spine (lumbar or thoracic region) and femurs. Fracture can happen even in minor traumatic situations like an awkward turn or a weak blow.
Often, these fractures appear for no apparent external reason. With a pathological fracture, displacement of bone fragments can occur, which leads to functional disorders of the limb (if the fracture is localized on a long tubular bone) and neurological disorders (if the fracture is localized on vertebral structures), which significantly worsens the quality of life of the cancer patient.
A growing tumor and bone fragments can compress adjacent tissues.
With tumor compression, the oncologist develops increasing pain, weakness of muscle tissues, signs of impaired sensitivity appear, and in the terminal stages, dysfunction of the organs of the pelvic localization and paralysis occur.
If metastasis is observed in vertebral tissues, then cancer patients sometimes experience spinal compression. Usually a similar phenomenon occurs with metastasis to the thoracic vertebrae. Disorders caused by compression can develop gradually (if the metastasis is compressing) or acutely (with compression by a bone or its fragment).
Symptoms of compression occur suddenly. If such a sign is detected at its initial stage, then its reversibility (at least partial) is quite possible. If, however, the compression is inactive, then the paralysis becomes irreversible.
With timely therapeutic assistance, specialists manage to achieve a significant reduction in symptoms, although only 10% of cancer patients with paralysis can move independently after treatment.
How to identify bone metastases?
The most informative diagnostic method for detecting bone metastases is skeletal, which allows you to accurately determine the prevalence and degree of metastasis.
Such a procedure is able to find metastases in any part of the human skeleton. Moreover, detection of the spread of tumor cells is possible at the very initial stages, when obvious disorders in bone structures are just beginning.
With the help of X-ray examination, bone metastasis can be detected only at the stage of sufficient maturity of the secondary formation, when about half of the bone mass has already been destroyed.
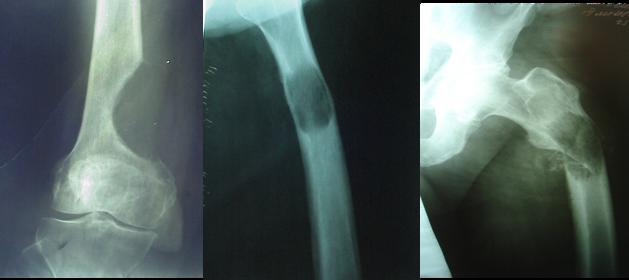
Photo of metastases in the hip bones on x-ray

But on the other hand, such a diagnosis allows us to differentiate a specific type of metastatic formation. Light white spots indicate blastic metastases, and gray-white spots indicate a lytic type of metastasis.
Radioisotope diagnostics or bone scintigraphy is performed using the Rezoscan radiopharmaceutical, which is administered to a cancer patient about a couple of hours before the scan.
Also, diagnostics may include either MRI, detection of resorption markers in urine, blood tests, etc. If metastasis is found in the cranial bones, then oncologists recommend carefully examining all organs to exclude the possibility of their damage.
Are they being treated?
Metastasis to the cranial bones is observed mainly in renal or thyroid cancer, and their treatment can be carried out by a variety of methods:
- Surgical interventions are performed during palliative therapy and are necessary for various complications (compression, fractures, etc.). After the operation, the pain syndrome is eliminated, bone marrow or limb functions are restored, etc.
- and in case of bone metastasis, it is used in complex conservative treatment, as well as in the preoperative or postoperative period. These techniques allow you to destroy cancer cells and prevent their growth.
- Treatment with bisphosphonates. These medications slow down the processes of disorders in bone structures.
- Radiopharmaceuticals, when administered, lead to the destruction of active cancer cells.
- involves the use of special means to increase the body's resistance, so that the immune system resists the spread of a tumor throughout the body.
Video about drugs for the treatment of bone metastases:
Treatment with bisphosphonate drugs
Bisphosphonates are medications that prevent bone loss. They are designed to suppress osteoclast activity and to prevent bone destruction.
At the site of growth of a secondary tumor, bisphosphonates are absorbed by osteoclastic cells, as a result of which they slow down or stop their activity. In addition, the use of bisphosphonates prevents the synthesis of osteoclasts, which become early dying or self-destructive.
Bisphosphonates are divided into 2 groups. One group of drugs contains nitrogenous compounds and is more effective against metastatic tumors. These include drugs like Ibandronate, Alendronate, Pamidronate, etc. Another group does not contain nitrogen, for example, Clodronate, Tidronate, etc. These drugs have a lesser therapeutic effect.
Bisphosphonate group drugs penetrate into bone mass, accumulate around osteoclasts and begin to oppress them, which leads to a decrease in the destructive activity of these cells. As a result, the processes of bone destruction are suspended.
Prognosis and life expectancy
The final prognosis depends on the location of the primary cancer.
- If bone metastases are formed from lung cancer, then the patient will live for about six months.
- If the primary focus is located in the prostate, then life expectancy will be about 1-3 years.
- If a cancerous tumor of the breast became the source of metastasis to the bone structures, then life expectancy will be approximately 1.5-2 years.
- Renal cancer with bone metastases leaves the cancer patient about a year of life.
- With bone metastasis, life expectancy will be no more than six months.
- With spread into bone tissue, life expectancy will be about 4 years.
Bone metastasis is extremely dangerous. If it is detected in a timely manner, then there is a high probability of saving the life of the cancer patient.
Oncological diseases of bones in modern medical practice are relatively rare. Such diseases are diagnosed only in 1% of cases of cancerous lesions of the body. But many people are interested in questions about why such a disease occurs, and what is the main symptom of bone cancer. After all, the sooner the diagnosis is made and treatment is started, the higher the chances of a successful recovery.
Unfortunately, the causes of primary malignant degeneration of bone and cartilage cells are still under investigation today. However, there is evidence that genetic inheritance matters in this case. In particular, genetic diseases such as Li-Fauman and Rothmund-Thomson syndromes increase the risk of bone damage.
On the other hand, oncological diseases can develop under the influence of external factors. In about 40% of cases, cancerous lesions of the skeleton develop after injuries and bone fractures. Exposure to radioactive radiation on the body, as well as poisoning with strontium and radium compounds, leads to malignant degeneration. Some people have developed cancer after a bone marrow transplant.
Classification of bone cancers
 In oncological diseases of the skeleton, the tumor develops either from bone or cartilage structures. In addition, the disease can be both primary and secondary. Primary cancer is most often diagnosed at a young and even childhood age. Secondary tumors are metastases formed by the migration of malignant cells from other sites of damage to the body. Bone metastases are possible with hemangioma, lipoma, reticulosarcoma, fibrosarcoma, etc.
In oncological diseases of the skeleton, the tumor develops either from bone or cartilage structures. In addition, the disease can be both primary and secondary. Primary cancer is most often diagnosed at a young and even childhood age. Secondary tumors are metastases formed by the migration of malignant cells from other sites of damage to the body. Bone metastases are possible with hemangioma, lipoma, reticulosarcoma, fibrosarcoma, etc.
In addition, bone tumors can be both benign and malignant (this is important, since the main symptom of bone cancer will depend on the nature of the neoplasm):
- A benign tumor has clear boundaries and most often correct form. Such a neoplasm is considered relatively safe, since it does not give metastases, although in some cases cells can be reborn. The processes of cell division and tumor growth are slow. Such diseases include osteoma and chondroma.
- Malignant neoplasms are characterized by rapid and aggressive growth. The tumor has no clear boundaries and easily grows into the surrounding tissues. Such diseases are often accompanied by metastasis and end in the death of the patient.
Benign bone tumors and their symptoms
 It is worth noting that most often such a disease is diagnosed at a young age (20-30 years), and men are more susceptible to it than women. As already mentioned, benign neoplasms are less dangerous, but this does not mean that treatment is not required here. So what is the first symptom of bone cancer?
It is worth noting that most often such a disease is diagnosed at a young age (20-30 years), and men are more susceptible to it than women. As already mentioned, benign neoplasms are less dangerous, but this does not mean that treatment is not required here. So what is the first symptom of bone cancer?
In fact, the initial stages of the disease in most cases are asymptomatic. Only in the later stages can some external signs. In particular, sometimes an uncharacteristic seal can be felt on the bone, which is perfectly felt through the skin. But pain rarely appears - the only exceptions are those cases when the neoplasm greatly increases in size, squeezing nerve fibers or blood vessels.
Sometimes the tumor grows so much that it is visible to the naked eye. But, importantly, the skin over the neoplasm does not change.
What are the symptoms of bone cancer?
The appearance of a malignant tumor is characterized by a more aggressive course, and therefore the clinical picture is more pronounced here. Pain is the main symptom of bone cancer. Patients often complain of pulling and aching pains, which can either be localized in the affected area or spread to other parts of the body (for example, if the shoulder is affected, pain can occur in the arm).
The intensive growth of a malignant neoplasm and the spread of metastases leads to depletion of the body, the onset of weakness, and a sharp decrease in weight. As in the previous case, the tumor can sometimes be felt through the skin, but it does not have clear boundaries. The skin over the affected area of the skeleton becomes pale and thin, and the translucent venous mesh gives the tissues a marble pattern. 
Leg bone cancer: symptoms and features
Approximately 60% of patients with bone cancer are diagnosed with osteogenic sarcoma. This is a malignant tumor that most often affects the tubular bones of the leg. A similar disease is diagnosed in adolescents and young people aged 10 to 25 years. In particular, such a neoplasm develops during a period of intensive growth and puberty, and boys are more prone to this disease.
As a rule, the tumor forms in the growth zone, for example, near the knee or at the lower end of the femur. Constant pain that gets worse when walking, temporary lameness, weakness, and sudden weight loss are the main symptoms of leg bone cancer. In the absence of treatment, metastasis occurs, and the lungs are primarily affected.
Pelvic bone cancer: symptoms and description of the disease
 The pelvic bones are most commonly affected by malignant Young's sarcoma. This disease is characterized by a malignant course, the rapid growth of the tumor and the spread of malignant cells throughout the body. As a rule, young people at the age of 20 years are more susceptible to the disease, although its occurrence is also possible in old age.
The pelvic bones are most commonly affected by malignant Young's sarcoma. This disease is characterized by a malignant course, the rapid growth of the tumor and the spread of malignant cells throughout the body. As a rule, young people at the age of 20 years are more susceptible to the disease, although its occurrence is also possible in old age.
Illness accompany characteristic symptoms. Cancer of the pelvic bones is accompanied by pain in the pelvis and thigh, which often spread to the entire lower limb. Soreness greatly complicates movement, so you can see that when walking a sick person is very lame.
Cancer treatment methods
There are many methods used to treat skeletal cancers. The choice of therapy here depends on the nature and size of the tumor, as well as its localization and the presence of metastases. A good effect can be achieved using radiation and chemotherapy. Ionizing rays, as well as chemical aggressive substances, have a negative effect on malignant tumor cells, eliminating not only the primary formation, but also its metastases.

In more severe cases, surgery is required. Surgical treatment is reduced to the removal of the affected parts of the bone and replacing them with metal implants. Naturally, further after the removal of the tumor, an additional course of chemistry or radiation therapy is required to neutralize the malignant structures remaining in the body.
What are the prognosis for patients with bone cancer?
Many patients are interested in the question of how long they live with bone cancer. There is no unequivocal answer to this question, since everything here depends on the nature of the disease, the stage of its development, the presence of metastases and the quality of the therapy performed. As a rule, benign neoplasms can be cured relatively quickly. Diseases of a malignant nature are much more difficult to treat. Nevertheless, with properly administered therapy, it is possible to achieve a stage of long-term remission (about five years). If the patient went to the doctor at the last stage of the disease, when the tumor had already managed to metastasize to the vital organs, the prognosis is not so favorable.
Cancer of the joints (hip, knee): symptoms
Alarms
The presence of such signs should alert a person and prompt him to seek medical help from a qualified specialist:
- The main, and often the only symptom, is pain in the affected joint or bone. Its appearance at rest and its gradual increase during daily activities should cause concern even in a skeptical person.
- The second symptom is the presence of a tumor-like formation. Cancer is characterized by the appearance of a dense, motionless, painful formation.
- Limitation of mobility and dysfunction of the limb almost always accompanies the previous signs.
With metastases, the signs are the same, but, unlike primary tumors, multiple and symmetrical lesions of large joints (hip, knee) are characteristic.
Symptoms in various forms of cancer
In clinical practice, up to 30 different types of malignant tumors of the skeleton are distinguished. The most common are neoplasms of bone, cartilage and connective tissues.
Ewing's sarcoma
It is characterized by a rapid course with a changeable, undulating pain syndrome. It is possible to detect a tumor during an external examination.
osteosarcoma
The knee joint is often affected. Characterized by intense pain in the affected area that occurs at night. Complicated by pathological fractures, metastases to adjacent formations.
Chondrosarcoma
This species is characterized by 2 flow options:
- Long-term, asymptomatic, with progression during the year.
- Fast, in which the development of the process occurs in a few months.
A characteristic clinical picture with the presence of all the listed signs. The pain is constant, with increasing intensity. The highest frequency of recurrence (recurrence of the process) is observed in this form.
fibrosarcoma
According to the results of observations, in 70–75% of cases, the process develops in the knee joint. The process is characterized by the following symptoms:
- Moderate pain that stops after taking analgesics.
- Prolonged course of the disease and late treatment to the doctor.
- A change in the shape of the joint with the formation of a soft tumor-like formation in its tissues.
Metastases
There is an uneven frequency of damage to organ systems. Tumors of the knee and hip joints are in second place in terms of occurrence after the bones of the spine.
Characteristic features of this type are:
- The pain syndrome appears several weeks earlier than other symptoms of metastases.
- Inconsistent nature of pain.
- Early (within a few weeks) appearance of radiological signs.
- Frequent complications (fractures, dislocations, bleeding into the joint cavity).
- A sharp deterioration in the quality of life.
- The need to take large doses of painkillers.
Diagnostics
Diagnosis on the basis of questioning and examining the patient alone presents certain difficulties. Complaints and external manifestations often mimic an inflammatory disease. The presence of symptoms of "fresh" or chronic injuries, which patients willingly report, can lead the doctor away from the correct diagnosis.
Thus, it is necessary to take into account not only the data of the clinical examination (localization, size, shape, consistency, soreness of the neoplasm). It is important to timely and accurately apply modern methods of radiological and functional diagnostics.
For diagnosis, almost any radiation methods can be used:
- X-ray of the joint in 2 standard projections (anterior and lateral).
- Magnetic resonance imaging (allows you to detect tumors from the connective and cartilage tissue).
- CT scan.
- Radioisotope study (the use of special particles that selectively accumulate in the tumor tissue).
- Positron emission tomography.
The confirmatory method is always a biopsy - taking a site of the primary tumor or metastasis for microscopic examination.
Forecast
Life expectancy after an established diagnosis depends on the stage of the process and the type of tumor.
After the therapy, it is necessary to observe the local therapist and oncologist for 5 years.
- In the first year of observation, a complete clinical examination is mandatory using laboratory and instrumental cell diagnostic methods every 3 months (quarterly).
- In the second year of observation, a survey every 6 months is sufficient.
- For the next three years, the survey is carried out once a year. It includes a complete blood count and a chest x-ray in 2 projections.
With modern methods of diagnosis and treatment, as well as timely seeking medical help, it is possible to save the lives of 80% of patients. With metastases, the prognosis is reduced to 50%.
Sarcomas are malignant tumors originating from cells of actively dividing connective tissue. Such tissue can be bone, cartilage, fat, muscle. Unlike other types of cancer, sarcomas are not attached to any organ and can form anywhere in the body.
Nevertheless, sarcoma has all the features characteristic of other malignant tumors - germination in neighboring tissues and their destruction, a tendency to relapse after removal of the primary focus, the formation of metastases in the lungs, liver, and other organs.
For sarcomas, in general, more rapid (sometimes explosive) and in any case faster growth than conventional tumors is characteristic - this is especially true for neoplasms that develop in childhood.
Consider what symptoms are in sarcomas of various localization.
Non-specific
Nonspecific symptoms of sarcoma are characteristic of tumors of any localization. Since toxic substances that are released during the life and decay of cancerous tumors poison the entire body, all systems and organs suffer. In addition, neoplasms form their own circulatory system which takes away nutrients and oxygen from other organs.
Sarcomas, as more aggressive tumors, can cause signs of general malaise of the body already at the initial stage of its development.
Nonspecific signs of connective tissue tumors include:
- pain syndrome in the area of localization of the sarcoma (pains with bone tissue sarcomas are especially painful);
- general weakness, lethargy, decreased performance;
- anemia (usually appears at the stage of tumor spread and is manifested by pallor of the skin, drowsiness, general loss of strength);
- decrease in the immune status of the body;
- the presence of an increasing neoplasm;
- lack of appetite (a symptom in particular for tumors of the intestines and stomach);
- fever, often not associated with infectious or inflammatory diseases, although infections and inflammatory processes also possible in the later stages of sarcoma due to weakened immunity;
- swollen lymph nodes;
- weight loss.
These signs are common to most cancers and do not specifically indicate the presence of a sarcoma. The diagnosis can be made only after a full examination in the clinic.
Specific
Specific symptoms relate to tumors of a specific localization and can be extremely diverse, since there are dozens of varieties of sarcomas. Signs of a malignant neoplasm depend on the location of the tumor or metastases in the body.
Osteosarcomas
Osteogenic sarcoma is a neoplasm with a high degree of malignancy. The tumor originates from the connective cells of the bone tissue and is characterized by rapid growth and a tendency to early metastasis. Symptoms of bone sarcoma depend on the location of the primary focus.
The most characteristic signs for this type of tumor are pain. They can be felt in the legs, arms and other locations of the focus of the disease. In most cases, sarcoma is located near the joints. At the onset of the disease, vague and indefinite pain sensations occur during movement and walking.
Symptoms of knee sarcoma - progressive lameness, change in gait.
On palpation of the affected area, severe pain occurs. Later, severe night pains are observed, which are not relieved by analgesics and do not subside even with fixation of the limbs. Similar symptoms develop with sarcoma of the lower leg, tumor of the thigh and the occurrence of neoplasms in the hip joint. With rib sarcoma, pain occurs when breathing and turning the torso.
Less commonly, sarcoma develops in the cranial bones and bone tissue of the upper and lower jaws. Symptoms of this type of tumor are: unsteadiness of the teeth, jaw deformity, violation of chewing functions. These types of sarcomas are also characterized by rapid growth and metastasis. In this case, secondary foci affect the brain, which usually leads to severe encephalopathy and death.
Gastrointestinal sarcomas
Sarcomas of the esophagus, stomach, and intestines begin with vague abdominal pain and signs of dyspepsia, then more pronounced manifestations develop:
- difficulty swallowing;
- internal bleeding due to perforation;
- intestinal obstruction.
Skin sarcomas
The initial signs of skin sarcoma are a single dense neoplasm, usually of irregular shape, protruding above the surface of the skin. The color of the tumor can be very different depending on the stage of the disease and its variety.
In the debut, the color may correspond to the skin, then the tumor darkens, its color becomes bluish or brown. As the tumor grows, it ulcerates, begins to bleed, and causes pain. Often there is inflammation of nearby veins and thrombosis.
Angiosarcoma
Angiosarcoma is characterized by damage to the vascular system. This is an extremely malignant tumor, sometimes developing over several weeks. Malignant cells originate from the vascular endothelium and can be localized in the lower extremities, mammary gland, and scalp.
Symptoms of this neoplasm:
Bone cancer: symptoms and treatment
Bone cancer is a group of malignant tumors that affect the skeletal system. This oncological disease is perhaps the most rare form of cancer. Bone tumors are most common in adolescents and children, and very rarely in the elderly. In adults, bone lesions are usually associated with metastases from another tumor (lung, breast, etc.)
Most common bone tumors: Ewing's sarcoma, osteosarcoma, chordoma, chondrosarcoma, fibrosarcoma, malignant fibrous histiocytoma
Ewing's sarcoma is considered the most aggressive bone tumor that occurs between the ages of 4 and 15 years. Men are most susceptible to developing this cancer. Ewing's sarcoma in people over thirty years of age occurs in isolated cases. The main localization of this tumor is the middle part of the long bones of the legs and arms. The prognosis of a three-year survival rate is about 65%, but it worsens significantly if cancer cells spread to other organs and tissues of the human body.
The most common primary bone cancer is osteosarcoma. which affects most often men in the age range from 11 to 24 years (older people are very rare). In children, osteosarcoma often develops in areas of intense growth near the knee and shoulder joints, as well as in the long bones of the legs and arms. This type of cancer is very aggressive and can spread to the lungs. The prognosis of five-year survival is about 65%
Chordoma- a rare tumor that develops in people older than thirty years (twice as often in men). Most often affects the upper and lower spine
Chondrosarcoma ranks second in prevalence (about 25%) of total number reported malignant bone tumors. These tumors develop from cartilage cells and can grow relatively slowly or be very aggressive. Chondrosarcoma is most common in adults over the age of forty (more often in men) and is prone to spread to the lymph nodes and lungs. The main sites of localization of this tumor are the hips and pelvic bones. The prognosis of a five-year survival rate for slow-growing tumors is about 90%, and for aggressive forms no more than 30%
fibrosarcoma is a very rare form of bone tumor that most often occurs in men between 35 and 55 years of age (slightly more common in men). The main localization sites are the posterior surface of the knee and the soft tissues of the legs.
Malignant fibrous histiocytoma is the most common soft tissue tumor in older people (over 50 years old) that affects fat deposits, tendons, ligaments and muscles. The severity of histocytoma can be different. The five-year survival prognosis is 45 to 60%.
Two more relatively common types of bone cancer can also be observed in a person: multiple myeloma and lymphoma. Multiple myelomas although they develop in the bones, they are not classified as bone tumors, as they are tumors of the bone marrow, not bone cells. Lymphoma- cancer, which usually begins its development in the lymph nodes from the cells of the immune system, but can also begin to form in the bones.
In addition to malignant bone tumors, various types of benign tumors can be observed: osteoblastoma, osteoma, osteochondroma, chondromyxoid fibroma, enchondroma, osteoblastoclastoma (often transformed into a malignant tumor)
Symptoms of bone cancer
The most common symptom of all bone tumors is pain. As the disease progresses, the symptoms become more severe. In the initial stages of tumor development, pain is most often observed at night, or during vigorous activity. Being directly dependent on the rate of growth of a malignant tumor, symptoms can be observed from several weeks to several years before a person seeks medical help. Sometimes swelling can be felt both on the bone itself and on the tissues surrounding it. Such manifestations are characteristic of fibrosarcoma and histiocytoma, but can also be observed in other bone tumors. Due to the development of a malignant neoplasm, the bones can weaken, which, with even minor injuries (or even their complete absence), leads to fractures. In addition, symptoms such as chills, fever, weight loss and night sweats can be observed, but they are less common, as they appear after the malignant process has spread to other organs and tissues of the body.
Diagnosis of bone cancer
X-ray examination is the primary diagnostic method of cancerous lesions of the bones. The presence of a bone tumor gives a fairly characteristic picture on the radiograph in the form of dark spots on the affected areas of the bone, or white spots on those areas where calcium deposits are formed as a result of the tumor process. A more sensitive method than X-ray examination is a bone scan, which allows you to detect even very small lesions that are not visible on the X-ray.
If the site of the primary tumor is already known, a biopsy is usually not performed for secondary cancer. If the exact localization of the primary lesion has not been established, a mandatory biopsy is shown to make the final diagnosis, which consists in examining suspicious cells under a microscope. In these cases, most often resort to a puncture biopsy, which is performed under local anesthesia. In some cases, an open biopsy is required, which is surgery performed under general anesthesia.
The rest of the tests are done to determine the spread of cancer cells (in the primary tumor), or to detect the primary lesion (the primary tumor is not localized, and the tumor being examined is secondary). Investigations include: MRI scan, liver ultrasound, chest CT scan
Treatment of bone cancer
The choice of tactics for the treatment of bone cancer primarily depends on the degree of prevalence and histological structure neoplasms. The main methods of treatment: surgical (radical) intervention, radiation therapy, chemotherapy. These methods are used both independently and in combination.
The most commonly used treatment for bone cancer is surgery, the goal of which is to remove the entire tumor and the adjacent healthy bone. The material obtained after removal is subject to careful study, the purpose of which is to determine whether normal bone tissue is present around the tumor. If any remaining cancer cells are found, further treatment is required. Not so long ago, the only option surgical treatment bone cancer was amputation, but modern methods of treatment have reduced its need to a minimum. To date, in most cases, the tumor is removed from normal bone without amputation. Based on the amount of bone removed, bone cement is used to repair the damaged area, or bone is transplanted from a bone bank or elsewhere in the body. In the case of significant lesions, metal implants are used, which can lengthen as children grow.
Radiation therapy is most commonly used for preoperative radiation. When it is carried out, high total focal doses are used. The expediency of combining radiation therapy with dimodifying effects (hyperbaric oxygenation, tourniquet hypoxia, hyperthermia) has been proven.
Chemotherapy for bone cancer is carried out before surgery to alleviate it and reduce the size of the tumor. It can also be used after surgery to kill any remaining cancer cells.
Popular materials
- Adrenogenital syndrome is a complex clinical and laboratory.
- Anasarca is a diffuse swelling of soft tissues with an advantage.
- Cholesterosis of the gallbladder is a pathological change in
- COPD is a common pathology of bronchopulmonary a.
- Hypovitaminosis is a pathological condition of the human body.
- Hypervitaminosis is an urgent acute pathological disease.
- Avitaminosis is a chronic pathological condition, fuss.
- Rheumatic heart disease is the most significant manifestation of rheumatic fever.
Joint sarcoma | Cancer - treatment and prevention
The main symptoms are quite traditional in these cases. As a rule, these are pain sensations, as well as a violation of the functions of movement. If the tumor is located in the cavity of the knee joint, then these symptoms are characteristic of all stages of the disease. Early diagnosis lends itself to sarcoma, which is close to the skin. At the same time, it protrudes, forming a bump, the skin changes color and, of course, such a sarcoma is easily felt on palpation. If the development of the disease has affected the tissues of the tendons and ligaments, then the limb completely loses the ability to move or perform any functions. The articular surface of the knee is also destroyed over time, leading to zero functionality of the leg. Pain increases, causing swelling, so there is a violation of nutrition, as well as blood supply to the lower leg.
Diagnosis and treatment
Synovial tumor of the knee and hip joint is diagnosed on the basis of x-ray or magnetic resonance imaging. The radiograph has several characteristic features, which manifest themselves as a symptom of Codman's triangle (this is when the tumor spreads throughout the bone), a symptom of a needle spicule (the tumor grows into the nearest organs) and spherical seals.
The treatment process involves surgery, in which a wide resection is applied (any lesions are removed). After surgical intervention chemotherapy, radiation therapy, or a combination of both. This allows to some extent to exclude the development of metastasis of the remaining cancer cells that cannot be removed.
Joint malignancy has a poor prognosis. Five years live on average about thirty percent of patients, even those who have undergone all types and methods of treatment. This is due to the fact that the tumor of the knee joint rapidly metastasizes.
The localization of the tumor is of great importance when choosing the nature of treatment.
Ewing's sarcoma is characterized by the following features:
- affects more often children;
- metastasizes to one or both lungs, as well as bones;
- amenable to radiation therapy.
This disease is very difficult to diagnose, so it is often confused with other types of diseases such as osteomyelitis or osteosarcoma.
Based on x-ray studies, some forms of Ewing's sarcoma can be distinguished:
- small-focal rounded destruction;
- lamellar destruction;
- macrofocal destruction.
The cent of such a tumor contains the so-called cavity with blood content. Most effective methods Treatment for Ewing's sarcoma is radiation and medication. The surgical method is rarely used, as it is considered ineffective. Operable treatment is used when the doctor is sure that this method is most suitable.
Sarcoma of the hip joint
The same rare malignant neoplasm is the sarcoma of the hip joint. On the contrary, it is more common in the male population. Symptoms this disease is this: sensations of dull pain in the pelvis and buttocks. Severe pain can cause short-term increases in body temperature. Increasing pain is characteristic of the progression of the disease. As a result of the development of sarcoma, a bump or swelling of the affected area may form. This process causes a significant thinning of the skin, so the vascular patterns are more visible. Late stages of the disease are accompanied by pain that manifests itself in the groin, thigh, spine and genital area. This is explained by the fact that the result of the growth of the tumor formation is the compression of the nerves and blood vessels. An increase in the size of the tumor provokes limitations in the functional abilities of the affected joint.
Sarcoma is a very serious disease, characterized by a rather painful course, therefore, drugs that have a narcotic effect are often prescribed to alleviate the patient's suffering. A large number of well-known diseases provide for certain preventive actions that are recommended to be carried out after the course of treatment, but this disease is not one of them. Everything that experts can recommend in this case, this does not apply to injuries and any damage to the joints negligently, but to engage in timely and complete treatment. People with a genetic predisposition should visit a specialist from time to time in order to make sure that the process of cell degeneration is excluded.
To the question "How and with what can one try to treat?" the doctor spread his hands.
replied that there were no drugs.
Would like a definitive answer:
Whether treatment in principle is possible or it is possible to give up as a bad job?
Registered: 10/23/2003 Posts: 3,684
For starters, provide a complete diagnosis!
(why did they do a scintigraphy?)
Registration: 04.04.2007 Posts: 14
Archipenko Ivan Grigorievi,
Ivan Grigoryevich! About two years ago, the same skeletal changes were found in me in Moscow. In the chest, humerus, cervical vertebrae, of particular intensity in the bones of the skull.
But he is still alive, and the pictures on Kashirka did not confirm the near-logical nature. I advise you to also turn to a good specialist - on the tighter Kashirka.
Sincerely, V. Serpukhovitin.
Archipenko Ivan Grigorievi,
During scintigraphy, the coefficient of accumulation of the radiopharmaceutical in the bone tissue should be indicated: in case of traumatic injuries or inflammatory diseases, it slightly exceeds the norm, and in case of metastases - significantly. Moreover, the norms of this coefficient may differ somewhat depending on the isotope and equipment used, i.e. standards need to be adjusted locally.
Registration: 09/07/2005 Posts: 967
- Now online
- Present: 0 users and 131 guests
- The record of simultaneous stay is 2,208, it was 09/23/2017 at 08:01.
- All Users not online
- Statistics
- Topics: 21,231 I Posts: 185,372 I Members: 53,434 I Featured
- Welcome new user, Glarina
Oncoforum.ru - information platform "All about cancer"
The site presents an extensive selection of materials on oncological diseases, their diagnosis, treatment and prevention, presented in an accessible form for readers. The most up-to-date and verified information is the news of world oncology about new drugs, methods of treatment and early diagnosis of cancer.
During the year, examinations are carried out in the department.
In our cancer community you will find support and support! We are ready to help you.
Features of skeletal bone scintigraphy: preparation for examination and diagnostic result
In diseases of the spine, joints, suspected development of a malignant tumor process, to control the treatment of oncopathologies, doctors prescribe skeletal bone scintigraphy. Small doses of radioactive preparations are used to assess the condition of hard tissues.
At low radiation exposure modern method diagnostics provides detailed information about the state of dense tissues throughout the body. The study has few limitations, deciphering the results allows doctors to timely adjust the treatment regimen, clarify the condition of problematic organs.
general information
During the examination, doctors perform functional imaging by injecting radioactive components to obtain a detailed image of all parts of the skeleton. To assess the degree of tissue damage, physicians determine the strength of the radiation of the administered drugs.
For the procedure, a complex device has been developed - a gamma tomograph. After a drip or injection of a radioactive substance, the patient is placed in a tomograph for reading using a gamma camera for the accumulation and distribution of a special drug in the skeletal system.
The procedure is multi-stage, the duration of the study is several hours. Despite some discomfort associated with the duration of the examination, the technique is often used by specialists of modern clinics to identify lesions in the early stages of cancer.
Types of skeletal scintigraphy:
- statistical. The doctor orders a limited number of images to clarify the morphological characteristics of a particular area. Comparison of different zones allows you to identify a malignant tumor process;
- dynamic. The doctor requires a series of images (continuous or with a certain period of time). It is important for a specialist to see the dynamics of changes in bone tissue. The frame rate is selected proportionally, according to the speed of the pathological processes that need to be controlled.
Advantages
Scintigraphy is an early diagnostic method. The radiographic behavior shows bone metastases when more than half of the dense tissue has lost functionality.
Unlike other methods, scintigraphy indicates a pathological process when the cells are in their normal state, but the functions are already impaired. Early detection of negative changes makes it possible to prevent advanced cases of oncopathologies due to the timely initiation of specific therapy.
Learn about the symptoms of degenerative - dystrophic changes in the thoracic spine and methods of treating pathology.
Instructions for using Diclac ointment to relieve pain in the back and spine are described on this page.
Despite the lower image clarity than with tomography (MRI and CT), a highly informative technique has positive aspects:
- simple preparation;
- low radiation dose;
- to monitor the results of treatment, scintigraphy can be performed even monthly;
- examination of all parts of the skeleton;
- accurate determination of single or multiple lesions, spread of metastases;
- effective control of the results of chemotherapy or the patient's condition after resection of the tumor or the problematic organ;
- the possibility of determining the degree of risk of recurrence after therapy of oncopathologies. Even in the absence negative manifestations for six months after irradiation and chemotherapy, the active capture of the radiopharmaceutical on the surface of the bones indicates a tendency to a recurrent pathology.
Indications for the study
Scintigraphy using radioisotopes is prescribed not only for the diagnosis and for monitoring the treatment of oncological diseases. Modern technique helps to identify many pathological processes in the skeleton in the early stages.
- diagnosis of complex fractures of the bones of the skeleton, if the x-ray did not show a clear picture;
- clarification of the causes of unexplained pain in the joints and spine;
- clarification of the risk of recurrence of the tumor process;
- diagnostic measures for suspected development of osteomyelitis;
- detection of severe pathology - cancer of the spine and bones;
- suspected osteonecrosis;
- clarification of the presence or absence of metastases in various organs. In most cases, without scintigraphy, it is difficult to determine how far the process of metastasis has gone. Only a complete examination of the bones of the skeleton using radioisotopes shows how the cancer has spread through dense structures;
- there are signs indicating the development of Paget's disease with a violation of the structure, deformation of the bone tissue;
- preparation for surgery to remove the mammary glands in a malignant tumor process;
- suspicion of the development of diseases, including infectious ones that adversely affect metabolic processes in bone tissue: tuberculosis, osteoporosis;
- the doctor suggests that the patient has thinning of the bone tissue (fibrous dysplasia).
Contraindications
A study using radioisotope preparations is not carried out during pregnancy. During the procedure, there is a potential risk of exposure to the fetus.
Skeletal scintigraphy should not be performed during lactation. If the child is breastfed, then you need to warn the doctor about the process. Sometimes, radiation diagnostics is indispensable in the presence of serious indications. In this case, scintigraphy during lactation is carried out, but after the study, the woman should not breastfeed the baby for another 5 days after the procedure, so that the remnants of radioactive drugs come out.
Before the procedure, doctors advise drinking more fluids. This moment is important for obtaining high-quality images and the speedy removal of the radioactive contrast agent from the body. The patient should temporarily remove the piercing, remove metal jewelry.
Special training is not needed, but to reduce the risk of errors, several types of drugs should be abandoned:
- beta-blockers for cores (substances accumulate in tissues, can reduce the clarity of images);
- iodine preparations - a month before the scintigraphy. You can not even lubricate the scratches with an alcohol solution of iodine;
- compositions containing bromine. This component often contains sedatives and cough mixtures.
How is the diagnosis carried out
- the first part of the procedure is the introduction of a contrast pharmaceutical preparation with a minimum level of radiation exposure. Next - a waiting period of three hours: the substance must get into all parts of the skeleton, be included in cellular metabolism;
- when the radiopharmaceutical has accumulated in the tissues, the patient takes the position of "sitting" or "lying down". A prerequisite for conducting high-quality diagnostics is complete immobility during the entire time of scanning the body;
- during the procedure, the patient is on a special moving table. A large crystal of the gamma camera registers radiation emanating from the entire surface of the body;
- the patient does not have to talk, but he hears the doctor, if necessary, transmitting commands from the next room;
- the examination is quite long, you cannot move while the scintillation crystal is working, which is not very convenient for children and seriously ill patients. To reduce nervousness, these categories receive sedatives (sedatives).
Preparations for skeletal scintigraphy
To reduce risks, doctors use ultra-short-lived and short-lived radionuclides. The components of specific pharmaceuticals act from several minutes to 5-6 hours. For scintigraphy of the skeleton, doctors use compositions based on fluorine, iodine, oxygen, carbon, and helium. Technetium 99 and indium 113 are obtained by the generator method.
The route of administration is intra-arterial or intravenous. The greatest accumulation of radioisotopes occurs in the skeletal foci, in which oncological and degenerative-dystrophic processes occur, as well as in the areas of metastases.
The main names of drugs for skeletal scintigraphy:
After the procedure
- at the end of the study, you must immediately remove the clothes in which the procedure took place, leave bandages, scarves, and cotton wool in the office so as not to take out items that have been exposed to radiation. To collect radioactive waste the clinic has prepared special containers;
- it is useful to drink more green tea, dried fruit compote, mineral water without gas, not very sweet fruit drink, rosehip broth for active removal of radionuclides with urine and sweat;
- after the examination, you need to take a shower, be sure to wash your hair.
View a selection of effective treatments for uncovertebral arthrosis of the cervical spine.
Read about the causes of pain under the scapula on the left side and options for treating discomfort at this address.
Possible Complications
Negative reactions depend on the general condition of the patient, the individual characteristics of the organism:
- allergic manifestations: skin itching, rashes like urticaria;
- itching and feeling of warmth at the injection site of the radiopharmaceutical;
- jumps in blood pressure, difficulty breathing, worsening of the general condition in severe forms of pathologies.
Deciphering the results
Doctors evaluate the data obtained from different angles:
- check the ratio of pulses over healthy areas and the lesion;
- identify the ratio of background activity to the number of impulses over the skeleton;
- identify metastatic foci, specify the degree of spread of cancer in distant organs.
After the examination, the doctor examines the images, if necessary, gathers a council to find out the opinions of other specialists. According to the results of bone tissue scintigraphy, the doctor prescribes treatment or corrects previously selected methods of therapy.
Price
To conduct the study, you need a modern SPECT / CT tomograph with a gamma camera. High-level inter-institutions and oncology dispensaries have the equipment. Skeletal scintigraphy is an expensive procedure: the estimated price of one study is up to four thousand rubles. Despite the high cost of the procedure using radionuclides, doctors strongly recommend undergoing an examination on a tomograph with a gamma camera for early diagnosis of severe pathologies.
Learn more about the advantages and features of skeletal bone scintigraphy in the following video:
- Ankylosing spondylitis (5)
- Hernia (18)
- Diagnostics (14)
- Other diseases (76)
- Intercostal neuralgia (7)
- Osteochondrosis (30)
- Symptoms (131)
- Spondylosis (7)
- Spondylarthrosis (7)
- Sofia - How to take coniferous baths: indications and contraindications for medical procedures for the treatment of pathologies of the pillar 1
- Anna - Most common causes pain in the neck and shoulders: treatment of discomfort with medicines and other effective methods 3
- Zoya Viktorovna - One of the important elements of therapy for diseases of the spine - chondroprotectors: a list of drugs to slow down the destruction of cartilage tissue 1
- Elena - The most common causes of pain in the neck and shoulders: treatment of discomfort with medications and other effective methods 3
- Elena - After the birth of a child, the lower back hurts 4
© 2017–2018 – Resource for the treatment of diseases of the back and spine
Copying materials is allowed only with the indication of the source.
The site is for informational purposes only. In no case do not self-medicate.
If you have any symptoms of diseases, contact your doctor.
About radionuclide IMAGING (scintigraphy) for a general practitioner
The first use of radioactive tracers dates back to 1911 and is associated with the name of György de Hevesy. The young scientist, who lived in a cheap boarding house, began to suspect that the leftover food, which he did not finish, was served to him again the next day.
The first use of radioactive tracers dates back to 1911 and is associated with the name of György de Hevesy. The young scientist, who lived in a cheap boarding house, began to suspect that the leftover food, which he did not finish, was served to him again the next day. He added a radioisotope tracer to the uneaten portion and, using a radiation detector, proved to his mistress that this was the case. The hostess kicked the young scientist out of the boarding house. He also continued his work, which resulted in the Nobel Prize for the use of radionuclides as indicators in biology. Radionuclide (radioisotope) diagnostics covers all types of applications of open radioactive substances for diagnostic and therapeutic purposes.
The clinical use of radiotracers came into practice in the 1950s. Methods are being developed to detect the presence (radiometry), kinetics (radiography), and distribution (scanning) of a radiotracer in the organ under study. Fundamentally new stage Radioisotope imaging is associated with the development of devices for a wide field of view (scintillation gamma cameras) and the imaging method - scintigraphy. Often, the term "scintigraphy" refers to studies conducted using both a linear scanner and a scintillation gamma camera. This terminological stereotype is associated with the formation of misconceptions about the diagnostic capabilities of the methods.
Scanning and scintigraphy are different methods of radioisotope imaging. Scintigraphy is significantly superior to scanning in terms of the volume and accuracy of diagnostic information. Modern scintillation cameras are computer-scintigraphic complexes that allow obtaining, storing and processing images of an individual organ and the whole body in a wide range of scintigraphic modes: static and dynamic, planar and tomographic. Regardless of the type of image obtained, it always reflects the specific function of the organ under study. Essentially, it is a mapping of functioning tissue. It is in the functional aspect that the fundamental distinguishing feature scintigraphy from other imaging modalities. An attempt to look at the results of scintigraphy from anatomical or morphological positions is another false stereotype that affects the expected effectiveness of the method.
The diagnostic orientation of a radioisotope study is determined by the radiopharmaceutical preparation (RP) used. What is RFP? A radiopharmaceutical is a chemical compound with known pharmacological and pharmacokinetic characteristics. It differs from conventional pharmaceuticals not only in radioactivity, but also in another important feature - the amount of the main substance is so small that it does not cause side pharmacological effects (for example, allergic) when introduced into the body. The specificity of the radiopharmaceutical in relation to certain morphofunctional structures determines its organotropism. Understanding the mechanisms of radionuclide localization serves as the basis for an adequate interpretation of radionuclide studies. The introduction of radiopharmaceuticals is associated with a small dose of radiation, unable to cause any adverse specific effects. In this case, it is customary to talk about the danger of overexposure, but this does not take into account the pace of development of modern radiopharmaceuticals.
Radiation exposure is determined by the physical characteristics of the radiotracer (half-life) and the amount of radiopharmaceutical administered. The present day of radionuclide diagnostics is the use of short-lived radionuclides. The most popular of these is technetium-99m (half-life - 6 hours). This artificial radionuclide is obtained immediately before the study from special devices (generators) in the form of pertechnetate and is used to prepare various radiopharmaceuticals. The values of radioactivity, introduced for a single scintigraphic study, create levels of radiation exposure in the range of 0.5-5% of the allowable dose. It is important to emphasize that the duration of the scintigraphic study, the number of images or tomographic sections obtained no longer affect the “set” radiation dose.
l Clinical application
Let us briefly dwell on the real diagnostic capabilities of the most common (“routine”) scintigraphic examinations.
Visualization of the skeletal system (osteoscintigraphy) is the most accurate method for identifying areas of impaired bone metabolism. Osteotropic radiopharmaceuticals (TC-phosphonates) have a high affinity for calcium phosphate crystals, so they bind predominantly to the mineral component of bone tissue. The level of accumulation of radiopharmaceuticals in various types of bones and parts of the skeleton is determined by the degree of osteoblastic and metabolic activity, the amount of blood flow, which must be taken into account when differentiating normal and pathological accumulation of radiopharmaceuticals. In particular, an increased accumulation of radiopharmaceuticals is observed in the metaepiphyseal sections of tubular bones, in areas with constant physical activity.
Bone diseases are accompanied by pathological restructuring of bone tissue, reactive or tumor bone formation - the main mechanisms that cause changes in bone metabolism and the accumulation of osteotropic radiopharmaceuticals in the affected areas. Depending on the combination of these processes, the level of accumulation of osteotropic radiopharmaceuticals increases in tumor, inflammatory, degenerative, and traumatic diseases.
The main and most responsible task of bone scintigraphy is the search for metastatic and assessment of the prevalence of tumor lesions of the skeleton. The scintigraphic manifestation of the pathology may appear 3-12 months earlier than the radiological signs appear. This is due to the fact that a local change in the exchange of osteotropic radiopharmaceuticals occurs in the early phases of the development of pathology, even before the appearance of not only radiological, but also clinical symptoms. For this reason, radionuclide research is most effective in pre- and postoperative examination of patients with tumors with a high frequency of bone metastasis (breast, lungs, prostate, kidneys).
Scintigraphic manifestation of metastatic lesions - multiple and less often single local areas of high accumulation of radiopharmaceuticals ("hot" foci). The highest concentrations of radiopharmaceuticals are observed in osteoblastic and mixed metastases, the lowest - in osteolytic ones. False-positive errors are most often associated with severe osteodystrophic changes, as well as traumatic injuries of the ribs and spine. Bone tumors of osteogenic origin are characterized by the highest accumulation of radiopharmaceuticals. For example, osteogenic sarcoma is characterized by pronounced hyperfixation of radiopharmaceuticals not only in the elements of the tumor itself, but also in the surrounding soft tissues due to reactive hyperemia (Fig. 1). In tumors of non-osteogenic origin, the accumulation of radiopharmaceuticals is lower. However, it is practically impossible to differentiate individual types of tumors according to the degree of accumulation of radiopharmaceuticals in them. Some tumors, as well as their metastases, may be the accumulation of radiopharmaceuticals. Such tumors include, in particular, reticulosarcoma and multiple myeloma. Visualization of the kidneys (dynamic renoscintigraphy) is a simple and accurate method for the simultaneous assessment of the functional and anatomical topographic state of the urinary system. It is based on the registration of the transport of nephrotropic radiopharmaceuticals and the subsequent calculation of parameters that objectify two successive stages.
Analysis of the vascular phase (angiophase) is aimed at assessing the symmetry of the passage of the "bolus" through the renal arteries and the relative volumes of blood flowing to each kidney per unit time. Analysis of the parenchymal phase provides a characteristic of the relative function of the kidneys (contribution to the total cleaning capacity) and the time of passage of the radiopharmaceutical through each kidney or its departments. Clinical interpretation is largely determined by the mechanism of RP elimination. Two types of radiopharmaceuticals can be used in dynamic visualization methods:
l glomerulotropic (DTPA derivatives), almost completely filtered by the glomeruli and reflect the state and rate of glomerular filtration;
l tubulotropic (analogues of hippuran) are secreted by the epithelium of the proximal tubules and reflect the state of tubular secretion, as well as effective renal blood flow. Indications for the study include urological and nephrological pathology, as well as diseases where the kidneys are target organs.
In different clinical situations, both the shape of the curves and their quantitative characteristics can change. However, it should be emphasized that the nature and magnitude of changes are not specific for a particular pathology and primarily reflect the severity of the pathological process. The greatest information content of renoscintigraphy is manifested in the differentiation of one- or two-sided kidney damage.
The leading sign that determines the side of the lesion is the asymmetry of the amplitude-time characteristics of angionephroscintigrams. The asymmetry of vascular parameters, and above all, the pronounced difference in the time of receipt of the radiopharmaceutical in the renal arteries, is one of the criteria for renal artery stenosis. The symmetry of changes in parenchymal function is more typical, in particular, for glomerulonephritis; asymmetry is a fairly constant sign of pyelonephritis, not only with one, but also with a bilateral process. Similar changes may accompany various types of anomalies of the kidneys and upper urinary tract (nephroptosis, doubling of the collecting system, hydronephrosis).
The method of liver imaging (hepatoscintigraphy) is based on the use of labeled colloids, which, after intravenous administration, are phagocytosed and distributed in morphofunctional structures containing RES cells in accordance with local values of organ blood flow. Normally, more than 90% of the administered radiocolloid is localized in the liver, about 5% in the spleen, and less than 1% in the bone marrow. Depending on the nature and severity of the pathology, these ratios change. The most common indication for hepatoscintigraphy is hepato- and/or splenomegaly of unknown origin. The main objective of the study is to differentiate the nature and clarify the severity of liver damage.
Diffuse liver diseases are manifested by changes in the size and shape of the image, the distribution of radiocolloid in the liver and its extraorganic accumulation, parameters of the phagocytic ability of RES and hepatic blood flow. It should be emphasized that the study does not allow to differentiate clinical or clinical and morphological forms of liver disease (for example, chronic hepatitis). The greatest information content of the method is manifested in the possibility of detecting portal hypertension syndrome (PHS).
Whatever the reason high blood pressure in the portal vein system (intrahepatic or extrahepatic forms), scintigraphically, LPH is manifested by high radiocolloid uptake and an enlarged spleen. The combination of these features makes it possible to detect LNG with an accuracy of up to 98% (Fig. 2). Focal lesions of the liver, depending on their prevalence, are manifested by the presence of single or multiple defects in the accumulation of radiopharmaceuticals within one or both lobes of the liver (Fig. 3). In practice, the identification of areas where there is no accumulation of radiopharmaceuticals (“cold” foci) is often strongly associated with volumetric processes, most often of tumor genesis. This notion is false. Enough wide range diseases associated with the involvement of the liver in the pathological process, scintigraphically can manifest focal changes as a result of local hemodynamic or functional disorders (liver cirrhosis, amyloidosis, histiocytosis). It must also be remembered that some organ structures (abnormally located gallbladder, mammary gland) can "shield" the image of the liver and form the scintigraphic phenomenon of "pseudotumor". That is why it is practically impossible to differentiate the specifics of the focal lesion by the nature of the defect in the accumulation of radiopharmaceuticals without taking into account clinical information.
The possibility of detecting focal pathology also depends on the resolution of the gamma camera. Lesions less than 1 cm, as a rule, are not manifested scintigraphically.
Visualization of the biliary system (hepatocholescintigraphy) is based on the use of a series of hepatotropic radiopharmaceuticals, similar in their pharmacokinetics to dyes (bromsulfalein, vofaverdin). After intravenous administration, they bind to blood proteins, are absorbed by polygonal liver cells and excreted in the bile. The main advantage of hepatocholescintigraphy is the continuity of visual and quantitative registration of the process of radiopharmaceutical kinetics.
Visual analysis of a series of images reveals some organic changes in the bile ducts (dilation), gallbladder (deformities), as well as functional changes in the duodenum.
Analysis of the curves makes it possible to obtain quantitative criteria characterizing the absorptive-excretory function of the liver, gallbladder filling, the duration of the latent period after a choleretic breakfast, and the rate of gallbladder emptying. Dyskinesia of the gallbladder is differentiated on the basis of a change in the rate of its emptying (hypo- or hypermotor dyskinesia). It should be emphasized that the accuracy of the radiological assessment of the motor function of the gallbladder exceeds the radiological or echographic. This is due to the fact that when comparing the image areas of an organ before and after a fixed time after a choleretic breakfast, it is practically impossible to take into account the duration of the latent period of bile secretion and to single out the actual phase of gallbladder emptying.
Hepatocholescintigraphy is of limited value in the diagnosis of inflammatory pathology and gallstones. The primary task is to assess the severity of the violation of the patency of the cervical-ductal zone and the filling of the gallbladder. With complete obstruction of the cystic duct, the scintigraphic phenomenon of the "disabled gallbladder" occurs.
Visualization of the thyroid gland (thyroid scintigraphy) is carried out using Tc-pertechnetate and is based on the similarity in the behavior of iodine ions and pertechnetate. However, this similarity is observed only in the initial inorganic phase of intrathyroid transport. Pertechnetate, unlike iodine, does not pass into the organic phase, that is, it is not included in the composition of thyroid hormones. This feature excludes the possibility of its use in the postoperative search for metastases of thyroid cancer (the latter is carried out only with radioactive iodine).
Nodular lesions of the thyroid gland and differential diagnosis of clinically or echographically identified nodular formations of the neck are the most common indications for thyroscintigraphy. The main task of the study is to assess the degree of functioning of the nodes, identify solitary or multiple formations, establish the connection of the nodes with the thyroid tissue. Depending on the functional activity and the degree of accumulation of radiopertechnetate, the nodes are traditionally divided into "hot", "warm" and "cold". However, this division refers only to their scintigraphic assessment.
The term "hot" node refers to a situation where the radiopharmaceutical accumulates almost exclusively in the region of the node and does not accumulate in other parts of the organ. Such findings are characteristic of autonomous thyroid tissue, toxic adenoma, autoimmune thyroiditis, and congenital aplasia of the lobe. The absence of radiopharmaceutical accumulation in the surrounding tissue node is explained by the production of thyroid hormones by the autonomous node, which reduce the release of TSH and cause the suppression of normal tissue function.
Functionally inactive ("cold") nodes are characterized by the absence or a sharp decrease in the accumulation of radiopertechnetate. This less specific finding accompanies a wide range of pathologies: nodular goiter, colloid cysts, adenoma, nonspecific strumitis, and thyroid cancer in 15–25% of cases (Fig. 3).
The greatest difficulty is the identification of "warm" nodes. These nodes are considered as a kind of "hot", but unlike the latter, they lack or have a weakly expressed functional suppression of normal thyroid tissue. Because of this, the accumulation of radiopharmaceuticals in the nodes may not differ from the surrounding parenchyma and lead to false-negative interpretations of scintigraphy data.
most read
news
Specializations
fresh issue#02/18
Means mass media www.lvrach.ru Founder: Open Systems Publishing House LLC Editor-in-chief: Akhmetova I.B. Editorial email address:
Editorial phone number: 7 Age marking: 16+ Certificate of registration of the mass media of the online publication El. No. FSot dated July 14, 2015 issued by Roskomnadzor.


